Share This Article
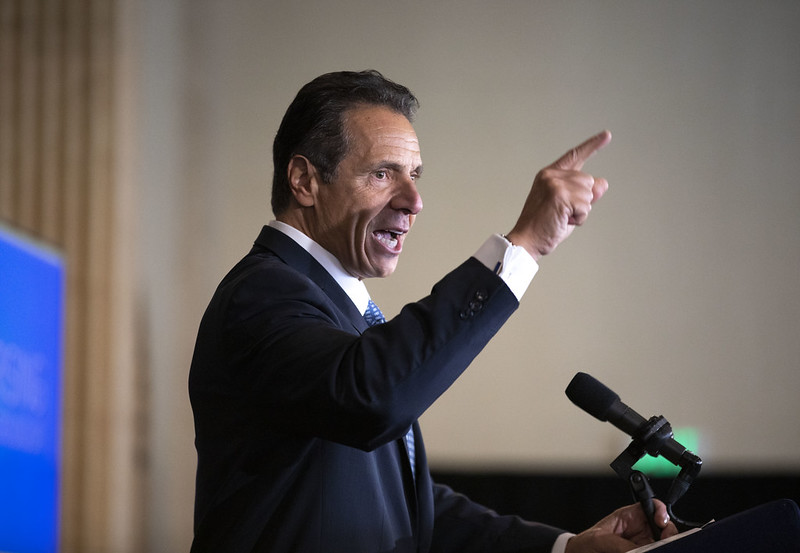
Office of the Governor
Advocates were critical from the beginning of the governor’s rushed Medicaid redesign timeframe, which left only eight weeks to decide upon the largest changes to the state’s Medicaid program in a decade.A series of far-reaching changes to New York state’s long-term care programs will limit enrollment in a program that is meant to give people with disabilities independence and which allows seniors to age at home.
With a home-health aide shortage and an aging population, Medicaid recipients fear they’ll no longer qualify for the Consumer Directed Personal Assistant Program, or CDPAP, and will be forced into assisted-living facilities and nursing homes this year when the budget takes effect. These fears are more pronounced now that nursing homes have become breeding grounds for COVID 19 cases.
“If I have to go to a nursing home or a hospital, that’s the end for me,” says Ed Sperling, a 69-year-old CDPAP enrollee who needs 24/7 care. Sperling is on the consumer advisory board of CDPAANYS, a group representing fiscal intermediaries, the companies that provide payroll and guidance to CDPAP enrollees.
Sperling is quadriplegic and has relied on CDPAP for nine years. He depends on a home-health aide whom he pays through CDPAP who helps him with grooming, showers, transferring him to a wheelchair and to a bed.
If he doesn’t qualify for CDPAP or his aide’s hours are cut, he said he fears he’ll have no choice but go enter a nursing home, where coronavirus infections have been spreading rapidly. This fear has been a topic of discussion in a weekly online support group he has been hosting since the outbreak.
As of Sunday March 29, 15 percent of COVID 19 deaths across the state were in nursing homes, according to the Department of Health. The facilities are so overwhelmed that some are urging family members to take loved ones home.
How we got here
In 2011 a Cuomo-appointed panel called the Medicaid Redesign Team mandated that adults on both Medicaid and Medicare, who need 120 days or more of long-term care, had toenrollin privately-run managed long-term plans (MLTCs.).The state also expanded a program called consumer directed personal assistance, or CDPAP, that was originally created to allow the disability community to live more independently.
CDPAP allows people with disabilities to hire their own home-health aides, which may include friends or family, and pay those employees with state money. CDPAP’s expansion to seniors was intended to cut costs by keeping people out of nursing homes and assisted living facilities, which also depend on Medicaidfunds.
But enrollment in MLTCs grew at a faster pace than the state was ready for, with 256,000 enrolled as of December 2019, up from 71,000 in December 2012. Late last year MLTCs, and CDPAP program specifically, were identified as the biggest cost-driver by the Cuomo administration in a $4 billion Medicaid overrun.
The nature of that cost overrun has sparked debate, however. The $4 billion represents spending that exceeded a mandatory cap on the state’s Medicaid growth, called the Medicaid Global Cap, created by the same Cuomo-appointed taskforce in 2011. Because the state’s Medicaid spending has exceeded that self-imposed growth rate, the state is now statutorily required to cut the program’s costs.
Alternately, the legislature could revise or repeal the Medicaid Global Cap, which was designed nearly a decade ago when the Affordable Care Act was still new and the state’s aging population had not yet begun to surge. It could then bring in any additional revenue needed to balance the budget by raising taxes, although the governor has rejected this approach.
Instead, he’s moved forward with stricter requirements created by a reconvened Medicaid Redesign team, including higher thresholds for daily care, new scrutiny of people who need care in excess of 12 hours, and caps on Managed Long Term Care growth.
Drivers of growth
In addition to a dispute over the cure (whether to cut the budget or lift the cap), there is also debate over the nature of the disease—in other words, over what has been driving the growth in CDPAP, with the Cuomo administration taking the stance that it is “inefficiency,” waste and fraud. For this reason, Cuomo announced in a January 21 executive budget speech that he’d be convening a new Medicaid Redesign Team, dubbed MRT II, to cut costs. A slide from his powerpoint displayed a shot from the 2012 film Marvel’s Avengers, along with a caption reading, “and they will be assisted by able crusaders,” when he made this announcement. The panel proposed different ways to cut enrollees, including increased scrutiny of who is eligible as well as tightened requirements.
But advocates believe that the growth of CDPAP is a result of the state’s aging population, Medicaid expansion under Obamacare, and a home-health aide shortage that left people with few other options. According to the Home Care Association of New York State, 17 percent of home-health aide jobs across the state are unfilled, and 24 percent of people who need a home health aide have trouble finding one. That shortage of home health aides is most pronounced in the upstate region, leaving people there especially to rely on CDPAP for care.
There has been little evidence that fraud or waste in CDPAP is pervasive or is driving the program’s growth. Rebecca Novick, an attorney at the Legal Aid Society who represents clients who need long-term care, says she hasn’t seen any examples of people in Managed Long Term Care plans or consumers in CDPAP who don’t need care.
“No, I’m not seeing it at all,” Novick says. On the contrary, she says, most of her clients are trying to get increased hours of care from private managed long-term care plans. She says Legal Aid is scrutinizing all the cases that come to them.
“We investigate these cases, speak to doctors, speak to family members, meet the clients,” she says. “These are situations of people only asking for the help that they need and having a hard time getting that and keeping that.”
However, the Medicaid Office of The Inspector General has found cases of fraud and recovered money for the program. Dennis Rosen, the state’s Medicaid Inspector General testified in a hearing in January the program was one of many Medicaid programs with issues.
“The program is so huge, there are going to be problems throughout,” Rosen said. “We get complaints on it, we also do audits on it. And we’ve had recoveries. That’s one of lots of areas where there are issues.”
All the advocates and attorneys who spoke with City Limits said that many people were essentially given no choice but to use CDPAP because of the homecare workforce shortage – people are allotted more hours if they use the CDPAP program because it does not require the state to hire from a pool of home-health aides that is scant to nonexistent.
“CDPAP is an excellent option for many people who want that, but it has been the only option for many people who otherwise can’t staff cases,” Novick says.
Fuzziness around the budget
The state’s budget negotiations ended with less transparency than any in recent memory, as legislators and advocates were mostly absent from the capitol due to the coronavirus outbreak.
In a Zoom press conference held on March 31, New York City Public Advocate Jumaane Williams criticized the governor’s decision to move forward with cuts. “Cutting Medicaid while people are dying would be a horrific choice,” Williams said. Williams and other advocates were in favor or repealing or adjusting the global cap and raising new revenue with an “ultra millionaire’s tax.”
One CDPAP consumer on the zoom conference call, Jessica De La Rosa, struggled to reconcile the governor’s heroic public image with the person sharply cutting services. “I hear him talking and how compassionate he sounds. He sounds like he really cares,” De La Rosa said. “And then I remember that he’s trying to hurt me and my people, and I freak out, because he sounds so compassionate.”
Advocates were critical from the beginning of the rushed Medicaid redesign timeframe, which left only eight weeks to decide upon the largest changes to the state’s Medicaid program in a decade. The MRTII panel voted on recommendations on March 19, most of which were included in the enacted budget, although some changes will be deferred so as not to jeopardize $6.7 billion in federal stimulus funding.
Among the recommendations from the panel that was included in the budget are a higher number of “activities of daily living” that are required to qualify for CDPAP. Consumers in the program will soon be required to need help with three or more activities of daily living. There is an exception for those who suffer from alzheimers or dementia, who are only required to need help with 2 activities of daily living.
The final budget increases scrutiny of “high utilizers” from CDPAP. More people who rely heavily on the program will be evaluated to to “ensure that it remains safe for that individual to remain in the community.”
The budget also sets a two-year moratorium on new Managed Long Term Care products, during which there will be a “wind down and elimination” of plans that aren’t integrated with Medicare. During this moratorium there will also be a cap on enrollment in MLTCs, enforced by the state’s withholding a percentage of premium reimbursement. (This cap is deferred until October, presumably to keep the state eligible for federal stimulus money that temporarily inhibits the governor’s powers over Medicaid.) It’s unclear how the cap will work, but it seems the expectation is that MLTCs, which are state regulated and privately run, will have to exclude more people from long-term care services in order to be fully reimbursed by Medicaid.
There will also be a longer “look-back” period for income eligibility in long-term care plans, so that the prior 60 months will be part of the income calculation. This means that people with higher incomes during the 5 year period preceding their application are less likely to be approved.
The MRTII panel also suggested eliminating a rule that allowed couples to meet the income threshold for Medicaid by allowing one spouse’s funds to not be counted toward Medicaid’s eligibility limit. The rule has been a bargaining chip in the state budget for years but when it was presented as part of the MRT II recommendations, advocates feared it was on the chopping block for real. To the relief of advocates this rule, referred to as “spousal refusal” ultimately went untouched in the budget.
There will be $45 million cut in wage reimbursements for CDPAP’s home health aides, which means these already low-paying jobs will face increasing pay cuts. “In the middle of a pandemic where every day (Governor Cuomo) is glorifying frontline healthcare workers, I thought that might go away,” Bryan O’Malley of CDPAANY said of the cuts.
Complex decisions in the teeth of a pandemic
In the final days of March, as the pandemic roiled New York City and the state budget was negotiated without rallies and protests that typically mark budget season, advocates pleaded with the governor and legislature to repeal the Medicaid Global Cap, a dated budgeting tool that nevertheless carries a legal mandate.
“We are currently at war with a pandemic. I would say yes we should repeal the Medicaid global cap,” Rosemary Rivera, Executive Director of Citizen Action of New York, told City Limits.
“A cap is just that, a cap. It does not care about pandemics,” Bryan O’Malley, who represents fiscal intermediaries in CDPAP, told City Limits. “It does not care about enrollment growth. The global cap is a blunt tool to control spending at any cost, and we are seeing that now.”
James Parrott, director of economic and fiscal policies at the Center For New York City Affairs, says the global cap has been used by the Cuomo administration for political cover. “That’s a totally unique Andrew Cuomo created artifact,” he says. The cap is not federally required. While the state government, unlike the federal government, must begin each fiscal year with a balanced budget, only the Cuomo-era cap mandates that cuts are made to Medicaid specifically.
Parrott says that the state should get its Medicaid costs under control, but doesn’t think the global cap has been applied well by the Cuomo administration to achieve this. For years, the Cuomo administration even deferred Medicaid spending to the following year’s budget in order to technically stay under the cap.
“It’s been applied in a way that allows him to exert more control,” Parrott says. “The legislature hasn’t come to grips with the governor’s control of the budget process.”
Not a question of whether, but where
For now, there’s fear that people who don’t have eligibility for home-based long-term care programs are more likely to end up in nursing homes or assisted living facilities, at a higher overall cost to the state and a higher personal cost to the elderly and disabled, who prefer to stay at home. Advocates said it was too soon to estimate how many, but the MRT II recommendations provide a glimpse at the state’s intent, as it carries dollar amounts. The panel estimated that all the changes to eligibility criteria for CDPAP, for MLTC plans and for other care services combined would save the state a $154 million in 2021 and $360 million in 2022. This suggests thousands could be omitted from long-term care plans and from CDPAP in the next few years.
Bill Ferris, New York State Legislative Rep for AARP, said that the organization has repeatedly asked their membership where they want long-term care, and the majority consistently answer that they want it in their homes. “They do not want to go to institutions,” he says. “If we want to save money, fill a gap, you’ve got to provide support to caregivers,” Ferris says. “You have also got to care for the individuals caring for the individuals,” Ferris said. An AARP analysis found that in New York, caregivers performed $31 billion worth of labor a year.
Ferris recommends investing in non-Medicaid community-based services, like a proposed caregiver tax credit, if the state wants to cut Medicaid growth.
“The alternatives to community-based support is nursing care, which is more expensive,” says Lara Kassell, coordinator of the group Medicaid Matters, who feels that the MRT II recommendations would force more people into facilities and cost the state more in the long run.
Rebecca Novick, of Legal Aid, says she believes some of her clients already struggling to get more hours could end up booted out of CDPAP altogether and forced into nursing homes.
“It’s not like the care becomes free,” Novick says. “Nursing homes are very expensive. Homecare can be very efficient.”
She says the characterization that friends or family shouldn’t be paid as caregivers ignored not just the savings to the state, but the day to day reality of caring for a loved one.
“It’s people who are working multiple jobs, trying to make ends meet, and taking care of their loved ones on top of that in hours that don’t exist,” Novick says.
1 Comment
Kathlyn McCormack
The Governor’s comments praising healthcare workers involved in the current pandemic is hypocritical when he is willing to cut Medicaid and effect healthcare workers who assist the elderly and handicapped so they can stay in their homes. The alternative of sending
these people into nursing homes is much more costly to Medicaid and is not emotionally better for them.
How can this even be considered? It makes no sense!
How would he like to see his mother in a nursing home when there is a better and less expensive alternative.