DeShaun Craddock
Brownsville, Brooklyn
This is the first part in Death’s Disparities, a series about the growing gap in life expectancy between rich and poor New York.
* * *
Scratch the surface of life in Brownsville, and chances are, the results will be less than healthy. By nearly any measure, life is harder, more dangerous and shorter here than in almost any neighborhood in New York City. Of Brownsville’s 17 elementary schools, 35 percent of students miss 20 days of school a year – that’s 2,786 children missing over a month of school every year, the highest rate of chronic absenteeism in the city. Of the rates of sugary drink consumption, new HIV infection and rates of death by heart disease, diabetes and cardiovascular disease, Brownsville leads or is among the hardest hit neighborhoods that the Department of Health and Mental Hygiene surveys annually for its Summary of Vital Statistics of New York neighborhoods.
To top it all, the neighborhood, a tiny quadrant of 2.1 square miles nestled in nearly the center of Brooklyn, has the dubious distinction of having the highest number of violent assaults in all of New York City.
It’s a difficult road, and Brownsville has been traveling it for decades: from high-density public housing to low concentrations of green space, from more trucks to fewer trees, from less healthy food choices to fewer paychecks – nearly everywhere you turn in Brownsville, barriers to healthy living abound, while opportunities to exercise, work or shop for fresh food are, for the most part, blocks away in other worlds.
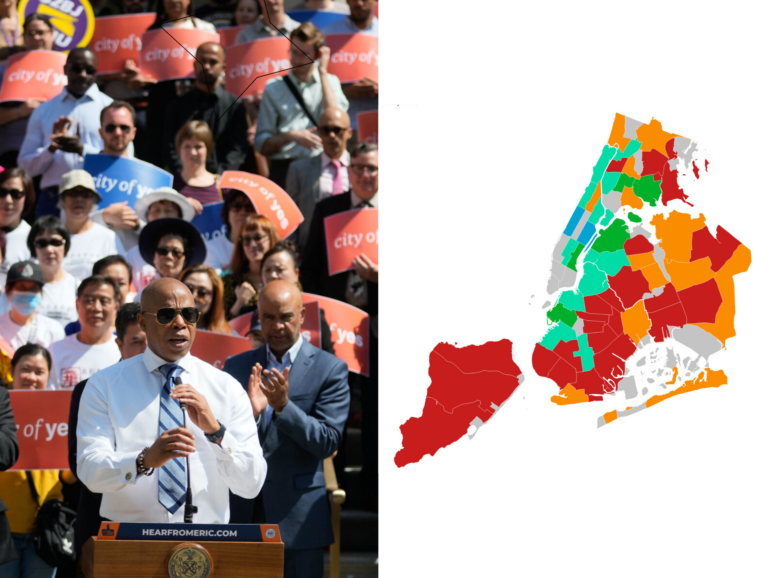
And the differences are striking: In the most recent Summary of Vital Statistics, an intensive, numbers-and-percentages look at the causes and rates of morbidity and mortality around New York City’s 59 neighborhoods put out every year by the Department of Health and Mental Hygiene, Brownsville, by nearly every metric, is consistently among the top 10 neighborhoods with the worst outcomes.
Not moving the needle
While citywide, life expectancy was up overall for New York City residents, with an average of 81.1 years, the gap between rich and poor neighborhoods grew from 2010 to 2014. In Brownsville, life expectancy in 2014 was lowest in the city, at 74.4 years. While citywide, infant mortality has dropped 30 percent since 2005, in Brownsville, the rate of infant mortality—while lower than it was a decade ago—is twice the citywide rate and four times greater than it is on the Upper East Side.
Among the city’s poorest neighborhoods—Morrisania, East Tremont and Mott Haven in the Bronx; East Harlem; and Brownsville and East New York in Brooklyn—rates of cancer, diabetes and cardiovascular disease remain firmly entrenched as leading causes of death. And deep in the Summary of Vital Statistics data are notes that make the reading even more distressing—like the fact that people of color living in high-poverty neighborhoods have lower rates of cancer than people living in wealthier neighborhoods, but are more likely to die of cancer, and die earlier, once it is contracted.
Thirteen years ago, the city Department of Health opened district health centers and located them in poor neighborhoods as a way for the department to better track community health. Now, all these years later, there is greater understanding about the health outcomes, but “we haven’t moved the needle around the disparity,” acknowledges DOH Assistant Commissioner Torian Easterling. Back in 2003, staff was deployed “to think about diabetes, stroke, heart attacks, the overlay of the crack epidemic and how they collect to health outcomes,” says Easterling.
“Fast forward 13 years, we have this information,” he adds. “What are the health outcomes? They are the same as they were 10 years ago.”
Yet there has over the past decade been change—substantial change—in the forces acting on neighborhoods like Brownsville and the health resources at hand in most of them. The 2007-2008 financial crisis hurt workers and also low-income homeowners. The waves of development and displacement that have contributed to the city’s homelessness crisis have increased the stress on many families with vulnerable health statuses. The Affordable Care Act has utterly the changed the medical landscape, in complicated ways. Hospitals have shut their doors, and Medicaid and Medicare have been reshaped significantly.
There have also been new, local efforts to deal with health disparities, like Take Care New York 2020 and the pledge in Mayor de Blasio’s OneNYC strategy to reduce premature mortality rates by 25 percent by 2040.
For now, the most pressing question is not only whether there is the sustained local political will to help struggling communities like Brownsville close the health and income disparities gap, but also whether the city and all its agencies working in concert will be able to sustain that effort, faced with the political and fiscal uncertainties looming in the changing landscape surrounding the election of the 45th president of the United States, Donald Trump.
The prescription
Most of the problems and issues surrounding negative health outcomes in high poverty neighborhoods have been known for a long time, says Humberto Brown, director of health disparities and new constituency development at the Arthur Ashe Institute for Urban Health in Brooklyn.
Health care is fractured in poor communities. There are few specialists willing to take Medicaid patients. There are immigrant or undocumented patients unwilling or unable to access the health care system for fear of repercussions. There are people resorting to their local emergency room because it makes more sense to sit there than wait four months for an appointment with a specialist.
And all those complications flow from pressure points – wage stagnation or joblessness, poor housing quality or homelessness, pollution – that are out of the control of the local community. “Most of the problems have been identified” but “you don’t see policies and initiatives to address them” says Brown, “they are studied and identified” and for the most part, nothing happens.
“We know now by most of the data, looking at social and economic conditions, the social determinants of health” – housing, employment, safety – “are much more impactful in higher degree on overall health than genetic or biological realities,” says Brown. If those factors don’t change—unemployment, unstable housing stock, buildings in disrepair, communities suffering from violence, lack of healthy food options, and clean, open air places to play—the levels of high negative health outcomes are unlikely to budge, he says.